My husband and I have been working on writing this article for a few weeks now. We have done our best to present this information in a way that gives the reader historical context and demonstrates these issues as endemic in for-profit-industry over the past century and beyond. The opinions we have expressed here are not only ours but are those of top historians (and others) who have been researching this issue for decades. If you have questions about anything you read here and would like additional information or links to other writings and research on the subject, please let us know. I suggest starting with reading the writings of world renown historians (and professors) David Rosner and Jerry Markowitz.
Section #1
Background & History
For more than a century, most Americans have been intentionally misled — through a false narrative carefully crafted and disseminated by the Lead industry via an incredibly successful “marketing” campaign (employing propaganda, political influence, and skullduggery) — to believe specific “facts” (myths) about childhood Lead-poisoning.
Why?
This effort has been undertaken to intentionally obscure the true size, scope, and impact of Lead-Poisoning — the single largest and most costly long-term public health crisis in this country — and to deflect blame and accountability for the incalculable ongoing harm done to successive generations of Americans from the Lead-based paint products (and, to a lesser degree, other Leaded products) these companies knowingly manufactured and promoted for decades evenafter their own scientists determined these products to be incredibly dangerous (harming employees of the companies but also causing permanent brain damage, seizures, and death to children exposed to even small amounts of the invisible toxic micro-dust continually coming off of surfaces in homes painted with Lead paint).
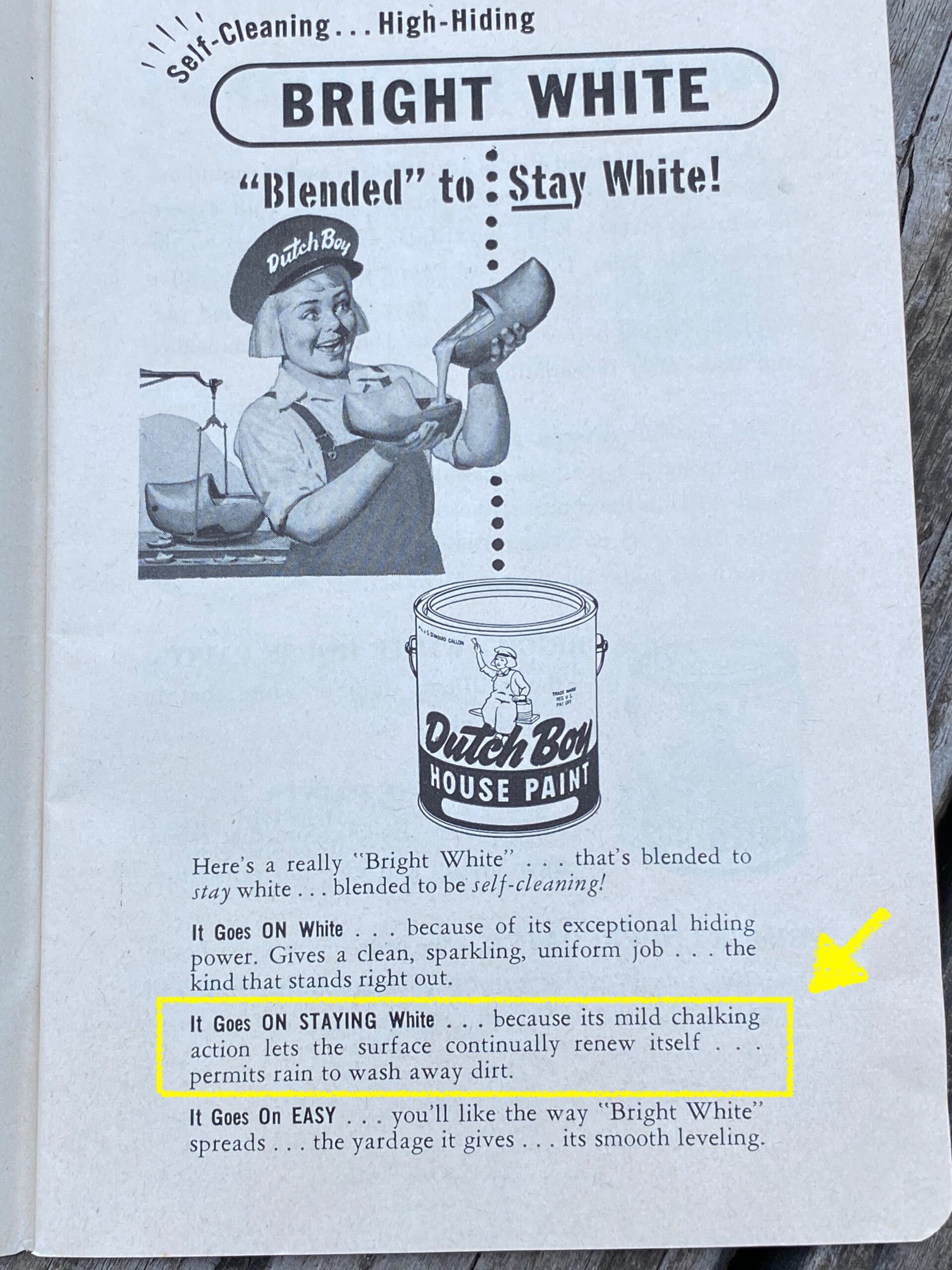
As you can see from the image below, the industry actually
promoted the dusting of these products as a benefit:
“… because its mild chalking action lets the surface continually renew itself…”
At the core of this false narrative are two key ideas
For most of the last four decades (since the “1978 ban on Lead paint”) if you randomly asked virtually any U.S. citizen what they knew about Lead-poisoning, you’d get an answer that contained various elements of this Lead industry-authored (or influenced) narrative. The two key misconceptions are as follows:
Lead-poisoning is mostly* a thing of the past, ‘solved’ with the 1978 ban on Lead-based paint.
Lead-poisoning “only” (primarily?) happens to low-income Black families, living in in poorly-maintained housing (“slums”).
*”mostly,” with the public consciousness exception being the situation in Flint.
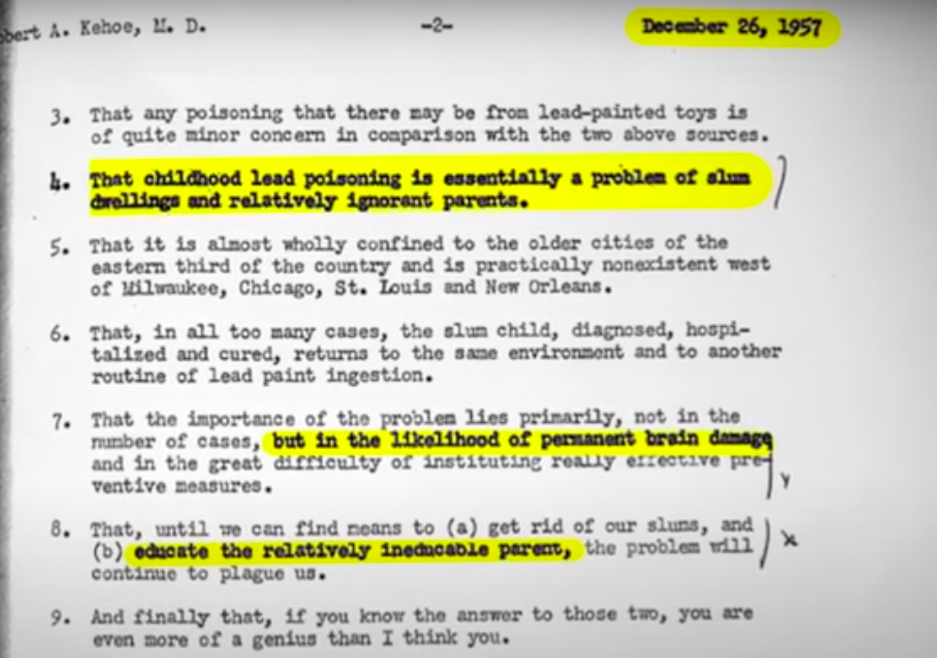
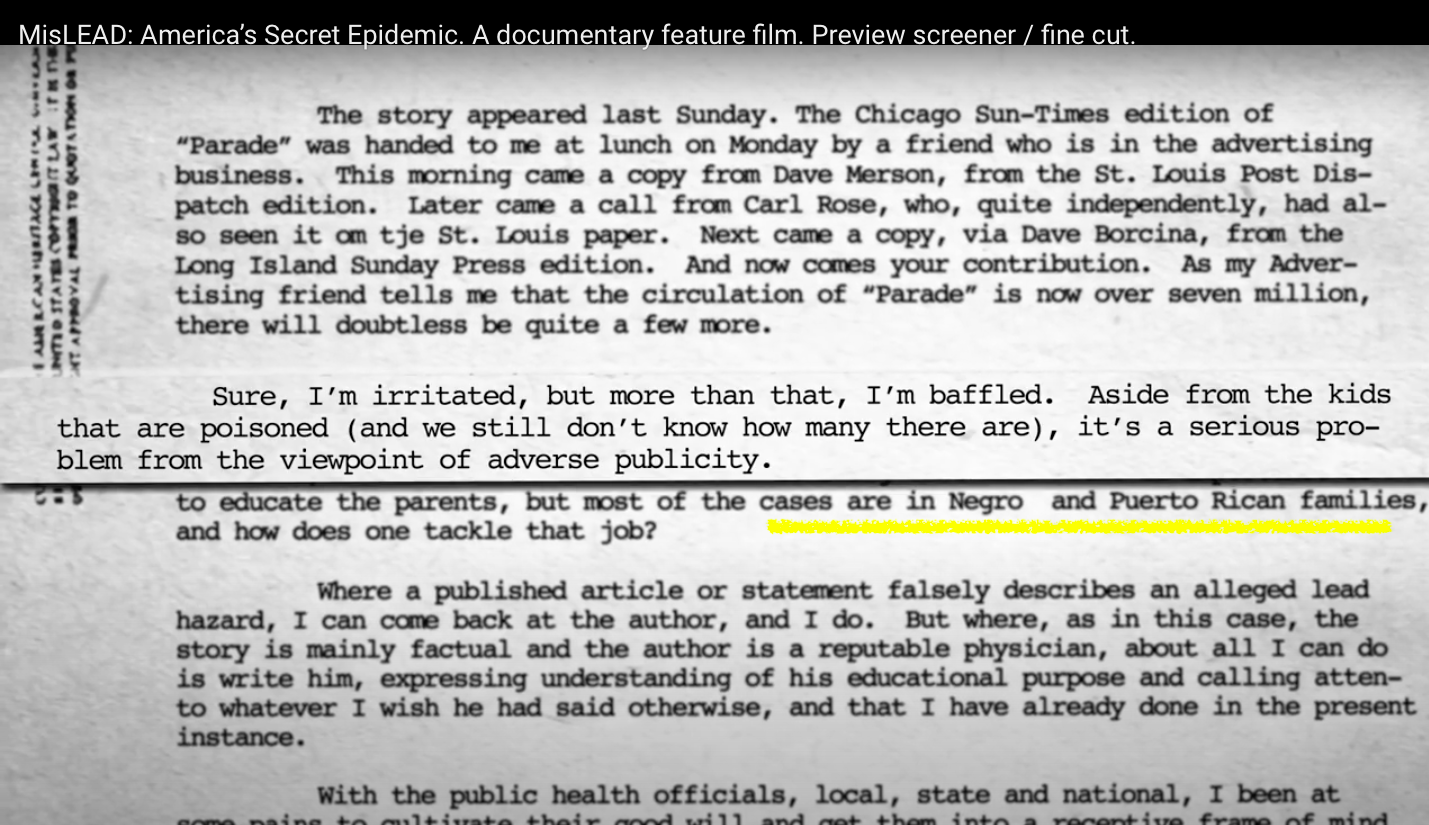
Neither of these “facts” are true; yet both are essential pillars of the strategic false narrative developed by Lead industry** marketing executives. This narrative was originally crafted in order to ensure that consumers (in the U.S. and abroad) would falsely believe that culturally-specific behavior (including alleged poor hygiene and poor home cleaning habits) of (“Negro” and “Puerto Rican”) “ineducable parents [the actual language used in Lead industry internal memos — see images below!]” was the cause of the Lead-poisoning of children.
As a result of these marketing initiatives (which date back to the early 1900s) historically, white families (today and in the past) have been led to believe that Lead-poisoning was not “their” problem or concern (ostensibly because they were educated and knew how to keep their homes clean).
The image below is a 1957 memo reiterating the popular thinking (based on the Lead-industry narrative that this was “essentially a problem of slum dwellings and relatively ignorant parents”).
Continue reading below the images.
Still image from the documentary feature film: MisLEAD: America’s Secret Epidemic
The Lead industry considered Lead poisoning an “adverse publicity” problem and set their marketing teams to the task of dealing with it:
Still image from the documentary feature film: MisLEAD: America’s Secret Epidemic
**Who is the Lead industry? Historically the Lead industry was made up of a handful of vertically-integrated companies — companies who mined, refined, and manufactured Lead pigment, and then turned that into Lead paint and other Leaded products. This included The National Lead Company (later the branding for their paint products was strategically changed to “Dutch Boy”); Sherwin Williams (their paint is still on our national monuments today — like the White House, and the “Hollywood” sign); Anaconda, Glidden, and a few other paint and product manufacturers. Even today (in 2020), the Lead industry (including many of these same original corporate dynasties) still exists and is thriving — reporting record profits year-over-year. (Read more at this link.)
As professors and historians David Rosner and Jerry Markowitz discuss, in their books on the subject, Lead-poisoning has been a racially-charged issue since the period of the American Industrial Revolution. In their research, they were able to obtain several of the original records of internal conversations and actual meeting minutes (including the documents in the images above) in which the Lead industry’s propaganda campaign architects discussed their concerns about “adverse publicity” caused by publicly shared incidents of children being poisoned by their products, and the need to combat this bad press by shifting public opinion based on a set of what some would now call “alternate facts” — made up to suit their own goals.
(It was really chilling to learn that some of these “p.r. architects” working with the Lead industry later were the very same people who ran the cloak-and-dagger “one-stop-shopping disinformation, fake science, and dirty politics” operations for the tobacco industry!)
Section #2
Racist Origins &
the Truth of the Matter
Lead-poisoning prevention’s racist origins
From the moment I learned that government funding could easily be allocated to eradicate childhood Lead-poisoning in our country but that the political will to do so did not exist (that the cost to eradicate the problem was a known quantity and was something our government had the capability to do), I began to learn how childhood Lead-poisoning was fundamentally a racist issue — but not in the way most people perceive it to be.
The top “layer of the onion”:
“What everyone knows…”
The surface understanding (the current/modern cultural manifestation) — or the top layer of the racism inherent in childhood Lead poisoning (and its prevention) today — is that “Lead poisoning is an environmental illness primarily impacting low-income Black families in America.” While it is true that there are many predominantly Black communities disproportionately impacted by Lead, that truth is actually only a small part of the story.
Who is actually “at risk” of being Lead poisoned?
Lead-poisoning is not caused by (nor dependent on) race, heritage, level of education, socio-economic status, or poor housekeeping. Lead-poisoning is primarily caused by Lead paint micro-dust – found in homes that were built and painted before 1978. Other sources of exposure include: Lead-contaminated soil, water, air, food, consumer products, and industrial or occupational exposure to Lead.
ANY man, woman, or child (any human, or any animal for that matter — livestock, wild, or pet!) who comes into contact with this incredibly potent neurotoxicant is potentially at risk. Lead does not discriminate; it is an “equal-opportunity poison.”
The second “layer of the onion”… Is that the first layer was an intentionally created myth — created so the Lead industry would not be held responsible for the financial repercussions of the human damage caused by their products:
The next layer to explore, in fostering a deeper understanding of the racism intentionally (and inextricably) woven into the issue of childhood Lead-poisoning (through the messaging crafted by Lead industry marketing “pioneers”) is the knowledge of the fact that it is specifically this well-crafted misperception (that “Lead-poisoning is predominantly a low-income Black problem”) that historically preventedlarge-scale, well-funded programs from being put in place to resolve this universal issue.
As long as this is perceived as being a predominantly Black issue, funding to solve it would not be allocated.
As long as this is perceived to be a predominantly Black issue, corporations who created the problem would not be held accountable for their actions.
The societal lack of value on Black lives historically, combined with the false narrative that this is restricted to being a “low-income, Black problem,” is the reason the issue of childhood Lead poisoning persists today.
Sadly, with systemic racism (officially unspoken/denied) being an ugly, but intrinsic organizing principle of our country and our government, as long as white, middle and upper-income families (and in particular, white, upper-income legislators and policymakers) believed this was a “low-income Black” problem (and not an urgent concern impacting their “demographic”), appropriate levels of funding would never be allocated.
As long as the people in power in our government and our communities felt this was “someone else’s problem” it would never be given the level of attention needed for this huge* national health problem to be resolved (and would forestall — for decades — the eventual revelation of the criminal activities of the companies who knowingly poisoned generations of American children for profit).
Section #3 Failings of the Public Health System
Continue reading below the image.
Still image from the documentary feature film: MisLEAD: America’s Secret Epidemic
The public agency role in holding systemic racism in place when it comes to Lead poisoning prevention initiatives:
The third “layer of the onion”… Public agencies cementing the Lead industry narrative in the public consciousness by parroting Lead-industry created myths in their programs and materials.
For half a century now, U.S. Federal agencies (EPA, CDC, FDA, HUD, etc.) have been complicit in reinforcing the Lead industry created stereotype, perpetuating the lack of funding for programs — through racist Lead-poisoning prevention marketing materials. It’s funny (to me as an activist) that the representatives of these agencies voice a persistent chorus of “we need more funding,” yet their racist actions (likely unintentional, but actions made within a culture of systemic racism) work against their goals — holding their limited funding in place.
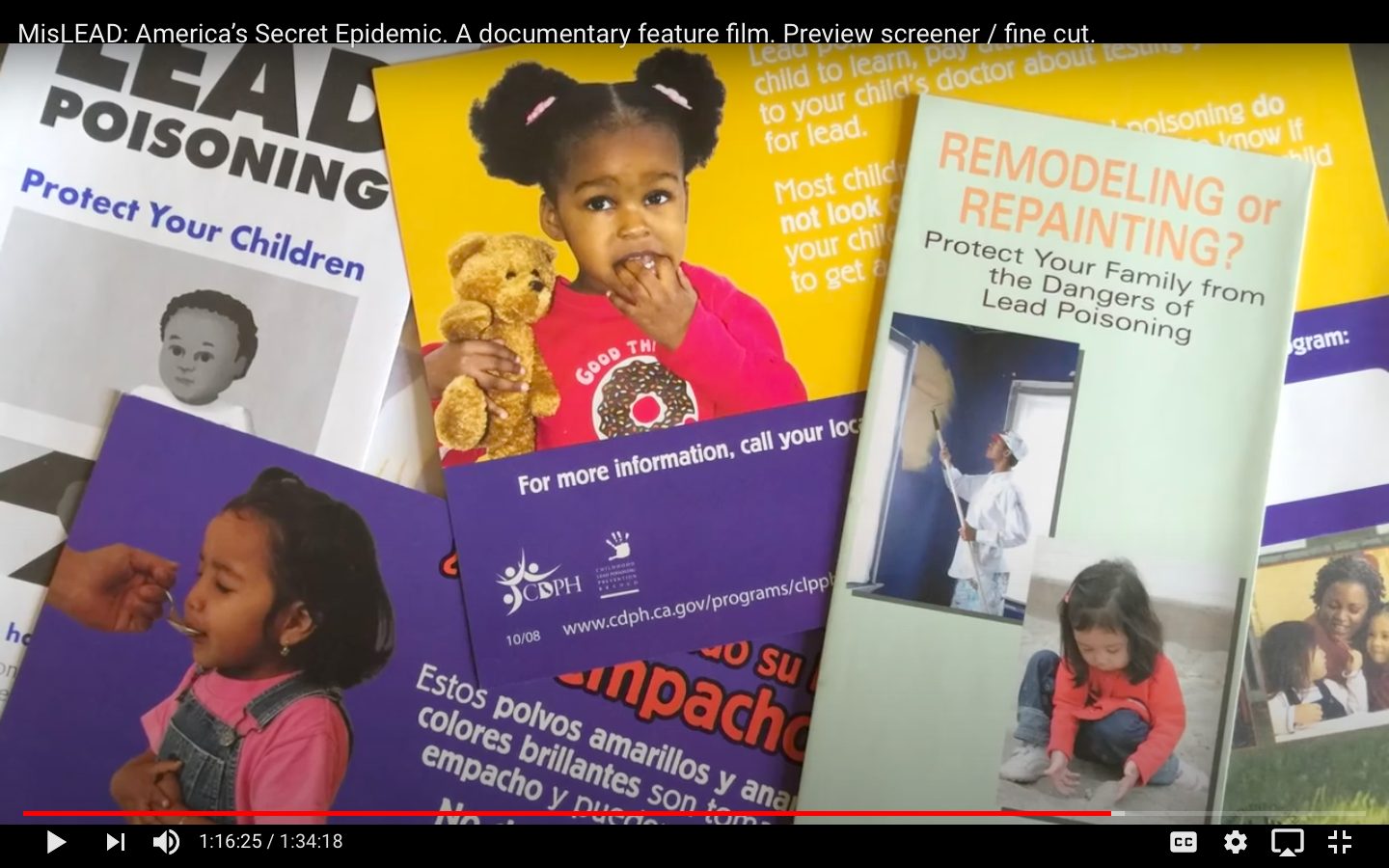
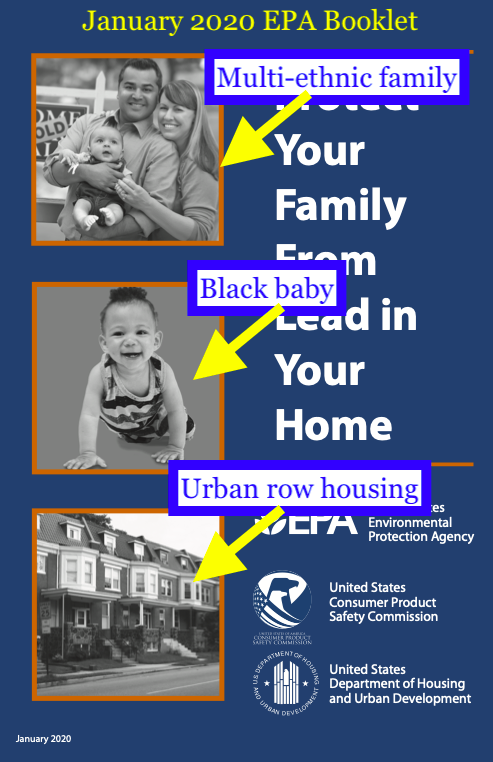
Reinforcing and perpetuating the Lead industry created narrative, the program materials from these agencies nearly always predominantly feature images of Black children (see image above and below). These government programs are also guilty of employing language focusing on Black communities (and specifically on negative stereotypes perpetuated by the Lead industry), with recommended courses of action that directly (and simultaneously “inadvertently”/ “passive-aggressively”) blame mothers for the problem (putting the alleged “solution” squarely in the mother’s realm of responsibility).
In holding these myths in place the programs then do next-to-nothing to actually help the impacted children (and even less to engage in their usual stated goal; truly focusing on primary prevention).
Continue reading below the image.
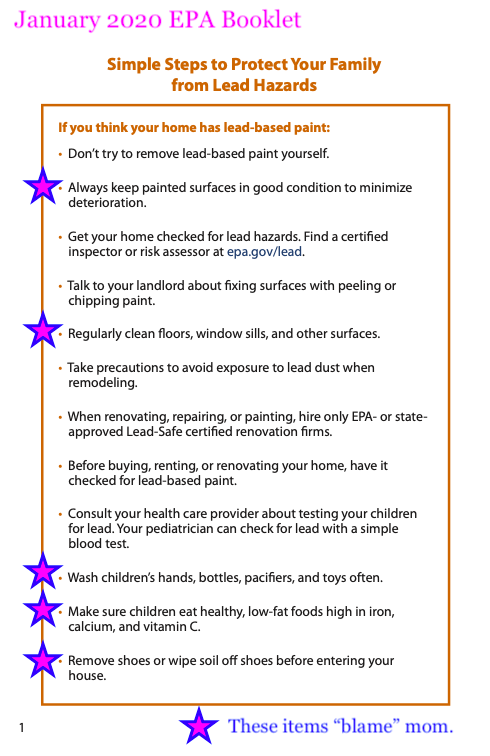
Specifically every program I have come across in the 15 years since my children were poisoned has recommended interventions focused on “teaching” improvedhousekeeping — implying that insufficient attention, time, or energy devoted to cleaning is the cause (or at least one of the main causes) of childhood Lead-poisoning. This is a Lead-industry narrative point. This is included (see EPA booklet page #1 below, from January 2020)despite a wealth of conclusive scientific evidence (as mentioned separately both by scientist Bruce Lanphear and former director of the National Center for Healthy Housing — Rebecca Morley — in my film) that poor housekeeping is not the cause of childhood Lead-poisoning, and that teaching mothers to clean their house better (with, for example, a “2-bucket” mop method for their floors or a “Swiffer”) does not eliminate the problem (and in fact, does next-to-nothing to protect children from being poisoned)!
Blaming mothers for their children’s poisoning by emphasizing their need to be better house cleaners may unexpectedly lead to MORE incidents of Lead poisoning because mothers get so exhausted from cleaning all the time (to keep up with the recommendations from public agencies to protect their kids, combined with the fear of CPS taking their kids away if they don’t clean well enough now that their child’s Lead poisoning is being monitored by the state) that they may accidentally overlook another potential exposure source.
The only true solution to childhood Lead poisoning is removing children (with their families!) from the toxic environment, or — better yet — making 100% sure that families with children (or expectant mothers, or grandparents for that matter) never move into a home with active or potential Lead hazards.
Continue reading below the image.
With 90% (+) of Lead poisoning prevention brochures depicting children of color, along with the focus of those brochures being that mothers need to clean their homes better, the public agencies that have created these brochures are playing right in the the blame-deflection-game crafted by the Lead industry.
In this way, the Lead industry has deflected blame for Lead poisoning and put the responsibility on the shoulders of mothers.
The fourth “layer of the onion”… Societal blaming of mothers (& specifically Black mothers)
This myth, the public perception crafted by the Lead industry at the turn of the twentieth century — that childhood Lead-poisoning is a “low-income Black” problem is discussed extensively in my film.
To recap:
Starting as early as the early 1900s, the Lead industry capitalized on the deep racist undercurrents in our country.
They harnessed systemic racism as a tool to deflect blame for their dangerous products.
Their marketing campaigns also claimed their products were “white” and “pure” (and therefore by association “safe”) and so the harm could not be the fault of the product.
They quite literally used racism to benefit and enrich themselves.
Industry specifically harnessed systemic racism to perpetuate the idea that “poor, ignorant Black women don’t clean their house well enough,” so “it’s only their children who are poisoned.”
Because Lead poisoning was therefore known to be a low-income Black problem, white women didn’t need to worry about Lead-poisoning (it was — by association then — asserted that white mothers have “superior” awareness/ education and know how to clean their homes properly). Since white families were thought to not be impacted, our predominantly white political base never allocated sufficient funding to solve the problem.
Through this narrative (and injecting elements of this narrative into our culture with an aggressive marketing campaign) the Lead industry protected themselves from the financial liability for the health impacts caused by their products (“health impacts” that included permanent brain damage, seizures, and death).
Shaming and blaming mothers for poisoning their children
This brings me to another aspect of the effects of the inherited shared racist narrative: Inherent shame — instilled by the (intentionally-harnessed and fostered) racism around the issue of childhood Lead poisoning.
Today, when most mothers learn their child has been poisoned many choose tonevereven speak of it (especially publicly!). A mother’s immediate reaction is to feel shame, even if they don’t fully understand why. Their cultural understanding of the issue (whether conscious or subconscious) makes them blame themselves for their child’s poisoning.
They blame themselves for not cleaning enough.
They blame themselves for not noticing hazards.
They blame themselves for moving into an unsafe home.
Yet none of this is their fault — their child’s Lead poisoning is 100% the fault of the Lead industry knowingly selling toxic products for decades upon decades and insisting they were safe.
I understand and appreciate this perspective (of self blame) and the concern for what others might think of you once your children have been poisoned. I understand this both from my personal experience and from my experience working with thousands of mothers of Lead poisoned children over the past decade and a half, as well as from my understanding of the history of the issue. After all, we were all raised to believe that childhood Lead-poisoning “is caused by poverty, ignorance, and/or parental neglect!” Whether consciously or not, given the (incorrect) understanding that Lead poisoning is a personal parenting failure, it’s too confronting for many families.
Many families choose not to become advocates for childhood Lead-poisoning prevention because of the extreme amount of cultural stigma and shame in having a Lead-poisoned child. As such, it was not easy to find families to be interviewed for my film** — putting your personal story out to the public can be confronting and frightening. Sharing about the Lead-poisoning of your children in a very public way (like in a news story or film) takes a certain mettle — as it can actually generate judgmental backlash (political and personal) against your family. This backlash can come from immediate family (grandparents, cousins, aunts & uncles) and from the greater community. This cultural shame around Lead poisoning is solidly rooted in racism, but that, too is by design.
**I am especially grateful for all the families who agreed to have their stories shared in my film. Many families I asked to participate refused, citing their shame over being responsible for their child’s poisoning — and fear that their friends and families would harshly judge them if their situation were made public.
Our public health programs should be helping families with this issue, but they are not. Why is this? Who is the public health system designed to benefit?
Given the date this article was published (Tuesday, July 21, 2020) I would be remiss in not noting the correlations between the epidemic of Lead poisoning in this country and the COVID-19 pandemic.
Our “leaders” are suggesting we stop testing. This has also been the case with Lead poisoning. Testing will show the true scope of the problem. Ceasing testing (because so many children are “testing low” now) will result in less pressure (in theory — as presented by rich white politicians) to allocate the necessary large-scale initiatives — and commensurate funding — to solve it permanently.
Elderly, low-income, and communities of color are being disproportionately impacted — primarily because they are prevented from having access to financial resources to address basic health, housing and safety concerns to keep them safe and healthy.
A lack of political will is generating a situation in which funding is not being appropriately allocated to resolve the problem quickly because the perception is that the people being impacted are “them” (not us) — with divisions along racial, socio-economic (and in the case of Covid-19, age) lines.
Those are just a few of the highlights of parallels between the epidemic of childhood Lead poisoning in this country and the COVID-19 pandemic. What these parallels demonstrate is that, fundamentally, public health is not a concern of our government and that public health is seen as a racially-divided issue.
Public health initiatives should benefit everyone
In most other “developed” countries (Finland, Norway, Denmark, England, etc.) public health resources are for all people. Public health is seen as a national priority. In America today (and historically), public health has been regarded as a (controversial) “last resort” intended only to (minimally) support low-income families and families of color — and again, it is our politicians using systemic racism to influence politics and “conserve” (redirect) tax revenue and other public resources that should be available to everyone.
Since these issues are not proportionately impacting our politicians directly (as most of them are old white men in the 1% and can afford Lead-free housing, for example), appropriate funding is simply not being allocated.
Section #4
The Influence of Old White Men
How do we get past this — and protect all the children?
Once I understood the basic principals behind the racist origins of the pervasiveness of childhood Lead-poisoning in America today (probably a year or two after my own kids were poisoned), I connected the dots and came to this unpleasant but pragmatic conclusion (which I mention often in my public speaking): in the U.S., because systemic racism is the foundation of the inaction (and specifically the foundation of the lack of proportionate, swift, comprehensive action) on the issue, the best way we can get childhood Lead-poisoning HANDLED (once and for all) would be to subvert the dominant and long-held messaging — by finding an older, white, male politician whose ownchildorgrandchild has been acutely and significantly Lead-poisoned!
(While this may perhaps no longer be true, given the emergent revolutionary political and social climate surrounding the issue of racial justice and racial equality today) I have long believed that the only way we (advocates, parents, activists, communities) can effect real change will be if we can find someone in a position of power who has a personalconnection to this issue — and can bring a new perspective — through insight about the true universal scope of Lead-poisoning to the political arena.
In theory, that person would have the power to bring the story to other politicians… “This is not just a problem for ‘them’ [the mythical “others” we have been led to believe to be the only ones who are “at risk”] — this is OUR problem; this an everyone problem — impacting all of the children and future generations of American citizens (not to mention the broader societal impacts of Lead on education, the healthcare system and the education systems in our country). This is unacceptable, and we need to solve this immediately!”
Looking for the Holy Grail —
a rich white male politician whose child or grandchild has been poisoned
While this may be reallyconfronting for many — and may evoke an unsavory association/image of the dreadful stereotype “White Savior”— it simply is (or has been, historically) a fundamental truth of our current racist political system. If a powerful (usually white, male) politician does not take a cause under their wing, it is much less-likely to see appropriate funding allocated to swiftly resolve the problem at its root cause.
Case Study — Section #4.a. — Jim
The Virginia Graeme Baker Pool and Spa Safety Act — an example
A textbook example of the above “truth” is the case of the drowning of Graeme Baker — and the consequent legislation (fairly rapidly enacted) to prevent a tragedy like that from happening again.
In June of 2002 Graeme Baker died when the suction from a spa drain dragged her under the water. The Virginia Graeme Baker Pool and Spa Safety Act was proposed within 4 years of her drowning and enacted within 5 years. Within 6 years of her death, the act became enforceable law — requiring safety measures to prevent drownings — specifically, coverings on pool and spa drains were now universally required to prevent a tragedy like this from happening again. Baker was the granddaughter of former Secretary of State, James Baker, III.
*Using numbers published by the CDC, it can be clearly demonstrated that one in three American children (people under the age of 18) in the United States today has had a blood Lead level of 2.5 or higher in their lifetime. This is approximately 22,000,000 children. Federal agencies agree there is no safe level of lead exposure for a child. The scientific consensus is clear that even blood lead levels as low as 1.0 or 2.0 can cause irreparable harm in the form of neurological damage and physiological implications including reproductive disorders, increased risk of heart disease, and more. Read more here.
Case study — Section #4.b. — Jason
A.J.’s Law — Lead-Safe Schools
I experienced this hard reality (that a white male politician was needed to get laws passed, and ideally a republican) first-hand, about 10 years ago.
In 2010-2011 I wrote a law for the State of Oregon that would have required Oregon schools to not have Lead hazards. Against all odds, “A.J.’s Law” managed to actually achieve bipartisan support early in the legislative process. The unpredictable factor that helped achieve this was support from Representative Jason Conger (a white, male Republican)!
It turned out Representative Conger’s daughter had tested positive for Lead when she was a baby (when they lived back on the East Coast, years before). He thus had a personal reason to be drawn to the legislation I proposed (which would have made it mandatory for all Oregon schools and daycare centers to contain no active Lead hazards).
With contemporary U.S. politics being the often soul-sucking, exasperating process it is — the law was eventually watered down to nothing (instead of requiring schools to be Lead-safe, in the end, it merely resulted in the creation of a website about Lead hazards in schools. Even so, this website later disappeared)! However, without Representative Conger’s enthusiastic support, the law would not have gotten as far as it did in the process.
Case study — Section #4.c. — George (Sr.)
In 1990 it took the poisoning of a DOG (the dog of an older white male politician) to generate action.
As further evidence that it (apparently) takes a wealthy white male politician to effect change in our country, it took the poisoning of the Bush family dog at the White House (in July of 1990 — 30 years ago!) to “inspire” action to protect American children from being exposed to Lead in their homes (specifically Lead hazards caused by renovations). This is also covered briefly in my film.
The incident of Millie the dog being poisoned (due to unsafe repainting and renovations being done at the White House) is actually why the EPA RRP Rule — the current legislation governing Lead safety in residential renovation, remodeling, and painting — was proposed! The first meaningful legislation protecting the nation’s children from Lead hazards in their homes came about because a WHITE HOUSE DOG was poisoned?!
Until that time the myth created by the Lead industry — that “only Black children” were at risk of being poisoned (because of their supposed ignorant “ineducable” parents”) — was enough to drive our white male government away from doing anything to protect all of the nation’s children from Lead (in the real-world, a non-discriminating/ equal-opportunity potent neurotoxin). As an issue that “only impacted Black families” it wasn’t perceived to be enough of an issue to create legislation around, but when it impacted the President’s dog — it was time to act.
Case study — Section #4.d. — Bernie
What about Bernie Sanders?
Then (fast forward to 2016), I met Bernie and Jane Sanders…
I sat backstage at a rally (in New Hampshire in February 2016) and chatted with Jane for quite a long time; in that conversation, Jane told me that, “Bernie is passionate about the subject of childhood Lead-poisoning,” adding that the family personally knew children who had tested positive for Lead in their blood. Yet — in our conversation — she did not seem to show any concern over any possible long-term implications of those positive test results (for the children she knew).
In my opinion, Bernie and Jane did not regard that (the poisoning of the children they knew) as concerning because of Bernie’s long history as an advocate for childhood Lead-poisoning prevention (and the aforementioned systemic racism inherent in the limited and misleading generally-available/accepted “body of knowledge” that has informed governmental Lead-poisoning prevention programs in this country).
It is exceedingly probable Bernie and Jane (wrongly) assumed these children’s Lead levels were “fine” “ok” or “below the threshold of concern,” likely because Bernie started doing this work back when a child was officially considered “poisoned” with a BLL of 40 micrograms per deciliter — and consequently, that some children they knew had a BLL in the range of 4 or 5 or 6 micrograms per deciliter (positive for Lead, but definitely “less than 10”) did not seem to be especially concerning to them.
Plus (and here’s the racial bias part — and to be clear, this pervasive bias was NOT in any way articulated in our conversation but is a context supplied by societal history), as the enculturated understanding goes, “this isn’t a problem that affects middle-class white children,” so the conclusion is that even though these children tested positive for Lead in their blood, it is unconsciously assumed that they (by virtue of not being the “at-risk demographic”) will be fine. And yes, ironically, this is sometimes true — when children have white privilege and all that comes with it — there is a possibility that the outcome of their Lead-poisoning will not be as severe (or at least the life-long financial and time burden of the impact less obvious, correctly diagnosed, attributed, or more easily-borne) compared to a child from a less-affluent Black or other non-white family. “Fine” is a relative construct, however (you can read more about that here).
After I had that conversation with Jane, I was excited about the possibility that perhaps (in the 2016 campaign), Bernie might publicly share the fact that children he personally knew had tested positive for Lead — but alas (rather sadly predictably, from a U.S. political perspective), to my knowledge he never mentioned it during his public speeches in his campaign. He is obviously passionate about the issue — and perhaps that is in some part due of his personal experience — but I never heard him speak of it as a personal cause per se. Not once.
Now in this “post-George-Floyd” era, perhaps the voices of women and people of color will be heard on this issue and we will no longer need to wait for an “Old Rich White Man” to save the day! (I’m looking at you, A.O.C.!)
In Conclusion
To be clear, all of this is NOT to say that Lead poisoning does not impact Black families disproportionately in many areas — it absolutely does! This article is rather to un-conceal and direct attention to the documented sustained, deliberate, coordinated, well-funded efforts that have successfully influenced public perception and produced political inaction (the pure lack of political will for swift impactful change) in the area of childhood Lead-poisoning, and to connect the origins of this inaction to the systemic racism in our country.
Perhaps with this (new?) perspective we can work together to free public health issues (including childhood Lead poisoning) from systemic racism in this country and (eventually) shift political will enough to get the funding allocated to resolve the problems once and for all.
Thanks for being here. Thanks for reading and sharing this work.
Please watch the preview screener of the film (on YouTube) for a more comprehensive exploration of the issue: https://youtu.be/eRKlaC2EjL0
Tamara Rubin
#LeadSafeMama
#BlackLivesMatter
Filmmaker’s note:
PLEASE do take 92 minutes to watch the preview screener of my film on YouTube. Make time — I promise you that you will not regret the time spent. It is a REAL movie movie. It was made for theatrical release and has been very well received by test audiences. While it looks done to most audiences, it was never completed (due to the lack of finishing funds precipitated by my need to divert all my available funds and energy to defend my advocacy against false accusations that attempted to shut it down). The film has MUSIC DONATED BY THE WHO! It has music DONATED BY TOM WAITS! It has footage from my interview with NOAM CHOMSKY and footage from my presentation with BERNIE SANDERS in FLINT! It has interviews with families of Lead-poisoned kids across the country. It has interviews with experts, scientists, and policy makers across the country, too. Thank you. Link: https://youtu.be/eRKlaC2EjL0
If you appreciate my advocacy work, please consider making a contribution so Lead Safe Mama, LLC can continue doing what we do. We still have over $50,000 in unpaid legal bills from defending this work against false charges over the past 4+ years, and my civil rights case (in Federal court, against the State of Oregon) is not likely to be resolved for another year or more. Here’s a link to contribute in support of this work.Here’s a link with the full original filing of my civil rights case.
For those new to this website:
Tamara Rubin is a multiple-federal-award-winning independent advocate for childhood Lead poisoning prevention and consumer goods safety and a documentary filmmaker. She is also a mother of Lead-poisoned children (two of her sons were acutely Lead-poisoned in 2005). Since 2009, Tamara has been using XRF technology (a scientific method used by the U.S. Consumer Product Safety Commission) to test consumer goods for toxicants (specifically heavy metals — including Lead, Cadmium, Mercury, Antimony, and Arsenic). All test results reported on this website are science-based, accurate, and replicable. Items are tested multiple times to confirm the test results for each component tested. Tamara’s work was featured in Consumer Reports Magazine in February of 2023 (March 2023 print edition).
Celia S. Deschin Ph.D.
First published: April 1971
American Journal of Orthopsychiatry
Page 344
For too long, professionals in the sciences–physical* and social–and those in the helping professions have attributed to their research and clinical findings a neutral and apolitical character that these did not and could not have. In the January 1971 JOURNAL, the lead article in the THEORY AND REVIEW section (Elizabeth Herzog: Who should be studied?) and the lead article in the CLINICAL section (David A. Anderson: Public institutions: their war against the development of black youth.) both highlight the need for a critical rethinking of the role of knowledge (i.e., theory and practice) if, as professionals, we are to be of service to a country in crisis. In particular, we need to challenge the assumption that our practice is not based on theory, an assumption that prevents periodic assessment of whether the underlying theory is consistent and supportive of the professional goals to which we are committed.
The Herzog article makes in clear that the practice of focusing studies on blacks and, to a lesser extent, poor whites is based on the theory, never made explicit, that the problem lies with those studied. The Anderson paper provides an analysis of the racist practices of institutions that have it within their power to eradicate childhood lead poisoning; it makes explicit the theory underlying the role of these institutions, unmasking their pretense of powerlessness and exposing their guilt in the murder of black children. (In the case studied, hospital doctors also were reluctant to test, and then to tread for lead poisoning at a time when mass screening for the disease was in the news.)
Not infrequently the research of professionals in the social sciences and the helping professions serves to obscure and block solutions that the researchers are presumed to be supporting. A case in point is the research focus on pica ** as [end of free sample]
* Today’s pollution problem was surely foreseen by scientists in industry, who, like good military men, were content to take orders, since to raise questions might jeopardize their jobs.
** Pica is described as a “perverted appetite for non-food items such as dirt, paper, paint and plaster,” or as “the habitual, purposeful, and compulsive search for and ingestion of such non-food items as clay, plaster, laundry starch, putty, string, paint chips, paper, dirt, crayons, yarn, matches and cigarette butts.”1
This is ABSOLUTELY BRILLIANT AND EXACTLY what I was saying! (and more) Thank you for sharing this with me. It’s amazing! From April of 1971… I was not yet two years old and yet this was known. Now, nearly 50 years later, the same thing holds true yet everyone (especially our pubic agencies) has turned a blind eye to the possibility of exploring fault within the underlying theory on which they base their programs. I really love this. Thank you for sharing it with me, Kenneth! I am going to post the PDF of this separately.
The pica aspect aspect to the Blame The Victim approach to lead poisoning also implicates the mother:
Lourie, R., Layman, E.M., Millican, F., Sokoloff, B. and Takahashi, L., 1958. A study of the etiology of pica in young children: an early pattern of addiction. In Problems of Addiction and Habituation (pp. 74-86). Grune & Stratton, New York.
… In an attempt to understand why children ingest lead-containing substances the focus shifted from the management of lead poisoning to the etiology of pica. Although organic, cultural and socio-economic factors were recognized as operative in the etiology of pica, the major emphasis in this study was on the emotional components. …
… Pica may be dealt with effectively by psychotherapy involving mother and/or the young child so that early treatment of pica has important implications from the viewpoint of public health (prevention of accidental poisonings, etc.) and mental health (prevention of adult addictions). …
—————-
I think the bigger picture is that the manufacturers of toxic products were paying doctors to lie about lead poisoning. Blaming races, mothers and children was their modus operandi.
“No honest and competent expert witness can prevail against such testimony unless he is in possession of incontrovertible evidence to the contrary.”
Note that in the letter below “0.079 mg. of lead per 100 grams of blood (or as it is expressed in the record, .079 mg.%)” is now represented as 79 µg/dl. “0.10 mg./100 g” is now 100 79 µg/dl.
Mr. W. M. Pallies
Health and Safety Manager
ESB Incorporated
P.O. Box #8109
Philadelphia, Pa. 19101
Dear Mr. Pallies
I have gone over the information contained in the record of Reuben D. Shoemaker
which you forwarded to me, and have concluded that this would be a very difficult
case to defend unless you have other and better information than that contained
in the record. The point that would be hardest to deal with, in evidence of
the incorrectness of the diagnosis of lead poisoning, is the finding of 0.079 mg.
of lead per 100 grams of blood (or as it is expressed in the record, .079 mg.%).
In evidence of the likely significance of the finding is the record of the
analytical findings previously. The record gives values as high as 0.10 mg./100 g.,
from time to time, and other high results more recently. As you know, the analytical
error of the best methods is of the order of 0.01 mg./100 g. for samples of 10
to 15 grams of blood, and since this figure is not challenged, and appears to be
the only one given in the record, it may well be satisfactory evidence of significant
exposure, especially if the claimant had been out of exposure for a time. The
clinical work-up appears to have been reasonably good, and here again, unless you
have evidence that will challenge the findings severely, you are up against it.
To answer your direct questions, I am still available for medico-legal testimony
if I can arrange to obtain information that enables me to arrive at an opinion.
In industrial cases, whether those of compensation claims or those concerned with
civil suits, and in trials based on alleged negligence, I am prepared to review
the facts and to advise concerning the validity of the claims. My appearance in
such cases is dependent upon my being able to meet the date or dates set for the
hearing, after I have determined whether or not I can testify effectively and in
good conscience.
The efficacy of the testimony intended to counteract false or mistaken claims, in
the specific case, is based, to a considerable extent, upon the reputation of the
specific plant for freedom from dangerous types of exposure to lead. The more
specifically applicable feature of the defense is the evidence available in the
hands of the plaintiff, to demonstrate (a) that the illness complained of is not
lead poisoning, and (b) that it is due to some definitive, alternative type of
disease. Without these features, a plausible medical record from a physician or
medical group with good professional standing, in association with a reputable
hospital, is very likely to stand against any outside opinion.
I feel sure that you know these things, but I mention them for emphasis. No honest
and competent expert witness can prevail against such testimony unless he is in
possession of incontrovertible evidence to the contrary.
If you wish me to give further consideration to this case, you should obtain for
me such evidence as may be available to discredit the diagnosis of lead poisoning.
If it should turn out that no such evidence exists, I would consider that my
service to your people might well be that of reviewing the situation of your
plant, or plants, from the aspect of industrial hygiene and medical information,
and determining, if possible, what should be done about them.
Sincerely yours,
Robert A. Kehoe, M.D.
Professor Emeritus of
Occupational Medicine
I’m really disappointed in you for jumping on the “systemic racism” bandwagon. At a time when common sense Americans need to come together, you are joining those who are trying to drive us apart with the racism scam. American is the least racist country in the world. Black Americans have more freedoms and more opportunities here than in any other country. Thankfully, many blacks see this and take advantage of the opportunities they have. Sadly, some don’t. There are poor and disadvantaged in all races. I know from personal experience that white people can be very poor also. Coming from the south, I know from personal experience that racism exist towards all colors, including whites. Yes, racism still exists in America, but we have come a long way in correcting that problem. Please don’t be one to help perpetuate the “systemic racism” false claims. That only sets us back.
I”m a bit confused about the Bernie bit of your article. I think Bernie is a sincere man, and I’ve seen him in videos when he would visit homes in Michigan about water quality. Why did you pull in his name? Why the interpretations on what his wife did and did not say? I don’t think it is fair that you did that.
What’s incredible about this is that Health Canada has absurdly portrayed lead paint as “an American issue” that we don’t have here. I couldn’t fathom how they could take this stance, but this article made me realize that the lead industries work in portraying this as a “black problem” is the reason why. Health Canada’s view is really “We don’t have the same poor black demographics as the US so logically we do not have a lead paint problem.”








https://onlinelibrary.wiley.com/doi/abs/10.1111/j.1939-0025.1971.tb01121.x
Knowledge is Neither Neutral Nor Apolitical
Celia S. Deschin Ph.D.
First published: April 1971
American Journal of Orthopsychiatry
Page 344
For too long, professionals in the sciences–physical* and social–and those in the helping professions have attributed to their research and clinical findings a neutral and apolitical character that these did not and could not have. In the January 1971 JOURNAL, the lead article in the THEORY AND REVIEW section (Elizabeth Herzog: Who should be studied?) and the lead article in the CLINICAL section (David A. Anderson: Public institutions: their war against the development of black youth.) both highlight the need for a critical rethinking of the role of knowledge (i.e., theory and practice) if, as professionals, we are to be of service to a country in crisis. In particular, we need to challenge the assumption that our practice is not based on theory, an assumption that prevents periodic assessment of whether the underlying theory is consistent and supportive of the professional goals to which we are committed.
The Herzog article makes in clear that the practice of focusing studies on blacks and, to a lesser extent, poor whites is based on the theory, never made explicit, that the problem lies with those studied. The Anderson paper provides an analysis of the racist practices of institutions that have it within their power to eradicate childhood lead poisoning; it makes explicit the theory underlying the role of these institutions, unmasking their pretense of powerlessness and exposing their guilt in the murder of black children. (In the case studied, hospital doctors also were reluctant to test, and then to tread for lead poisoning at a time when mass screening for the disease was in the news.)
Not infrequently the research of professionals in the social sciences and the helping professions serves to obscure and block solutions that the researchers are presumed to be supporting. A case in point is the research focus on pica ** as [end of free sample]
* Today’s pollution problem was surely foreseen by scientists in industry, who, like good military men, were content to take orders, since to raise questions might jeopardize their jobs.
** Pica is described as a “perverted appetite for non-food items such as dirt, paper, paint and plaster,” or as “the habitual, purposeful, and compulsive search for and ingestion of such non-food items as clay, plaster, laundry starch, putty, string, paint chips, paper, dirt, crayons, yarn, matches and cigarette butts.”1
This is ABSOLUTELY BRILLIANT AND EXACTLY what I was saying! (and more) Thank you for sharing this with me. It’s amazing! From April of 1971… I was not yet two years old and yet this was known. Now, nearly 50 years later, the same thing holds true yet everyone (especially our pubic agencies) has turned a blind eye to the possibility of exploring fault within the underlying theory on which they base their programs. I really love this. Thank you for sharing it with me, Kenneth! I am going to post the PDF of this separately.
Tamara
Tamara
You’re welcome.
The pica aspect aspect to the Blame The Victim approach to lead poisoning also implicates the mother:
Lourie, R., Layman, E.M., Millican, F., Sokoloff, B. and Takahashi, L., 1958. A study of the etiology of pica in young children: an early pattern of addiction. In Problems of Addiction and Habituation (pp. 74-86). Grune & Stratton, New York.
… In an attempt to understand why children ingest lead-containing substances the focus shifted from the management of lead poisoning to the etiology of pica. Although organic, cultural and socio-economic factors were recognized as operative in the etiology of pica, the major emphasis in this study was on the emotional components. …
… Pica may be dealt with effectively by psychotherapy involving mother and/or the young child so that early treatment of pica has important implications from the viewpoint of public health (prevention of accidental poisonings, etc.) and mental health (prevention of adult addictions). …
—————-
I think the bigger picture is that the manufacturers of toxic products were paying doctors to lie about lead poisoning. Blaming races, mothers and children was their modus operandi.
“No honest and competent expert witness can prevail against such testimony unless he is in possession of incontrovertible evidence to the contrary.”
Note that in the letter below “0.079 mg. of lead per 100 grams of blood (or as it is expressed in the record, .079 mg.%)” is now represented as 79 µg/dl. “0.10 mg./100 g” is now 100 79 µg/dl.
https://www.toxicdocs.org/d/npR4MzrGZw39NKML5ov6L1y0G?lightbox=1
October 3, 1968
Mr. W. M. Pallies
Health and Safety Manager
ESB Incorporated
P.O. Box #8109
Philadelphia, Pa. 19101
Dear Mr. Pallies
I have gone over the information contained in the record of Reuben D. Shoemaker
which you forwarded to me, and have concluded that this would be a very difficult
case to defend unless you have other and better information than that contained
in the record. The point that would be hardest to deal with, in evidence of
the incorrectness of the diagnosis of lead poisoning, is the finding of 0.079 mg.
of lead per 100 grams of blood (or as it is expressed in the record, .079 mg.%).
In evidence of the likely significance of the finding is the record of the
analytical findings previously. The record gives values as high as 0.10 mg./100 g.,
from time to time, and other high results more recently. As you know, the analytical
error of the best methods is of the order of 0.01 mg./100 g. for samples of 10
to 15 grams of blood, and since this figure is not challenged, and appears to be
the only one given in the record, it may well be satisfactory evidence of significant
exposure, especially if the claimant had been out of exposure for a time. The
clinical work-up appears to have been reasonably good, and here again, unless you
have evidence that will challenge the findings severely, you are up against it.
To answer your direct questions, I am still available for medico-legal testimony
if I can arrange to obtain information that enables me to arrive at an opinion.
In industrial cases, whether those of compensation claims or those concerned with
civil suits, and in trials based on alleged negligence, I am prepared to review
the facts and to advise concerning the validity of the claims. My appearance in
such cases is dependent upon my being able to meet the date or dates set for the
hearing, after I have determined whether or not I can testify effectively and in
good conscience.
The efficacy of the testimony intended to counteract false or mistaken claims, in
the specific case, is based, to a considerable extent, upon the reputation of the
specific plant for freedom from dangerous types of exposure to lead. The more
specifically applicable feature of the defense is the evidence available in the
hands of the plaintiff, to demonstrate (a) that the illness complained of is not
lead poisoning, and (b) that it is due to some definitive, alternative type of
disease. Without these features, a plausible medical record from a physician or
medical group with good professional standing, in association with a reputable
hospital, is very likely to stand against any outside opinion.
I feel sure that you know these things, but I mention them for emphasis. No honest
and competent expert witness can prevail against such testimony unless he is in
possession of incontrovertible evidence to the contrary.
If you wish me to give further consideration to this case, you should obtain for
me such evidence as may be available to discredit the diagnosis of lead poisoning.
If it should turn out that no such evidence exists, I would consider that my
service to your people might well be that of reviewing the situation of your
plant, or plants, from the aspect of industrial hygiene and medical information,
and determining, if possible, what should be done about them.
Sincerely yours,
Robert A. Kehoe, M.D.
Professor Emeritus of
Occupational Medicine
I’m really disappointed in you for jumping on the “systemic racism” bandwagon. At a time when common sense Americans need to come together, you are joining those who are trying to drive us apart with the racism scam. American is the least racist country in the world. Black Americans have more freedoms and more opportunities here than in any other country. Thankfully, many blacks see this and take advantage of the opportunities they have. Sadly, some don’t. There are poor and disadvantaged in all races. I know from personal experience that white people can be very poor also. Coming from the south, I know from personal experience that racism exist towards all colors, including whites. Yes, racism still exists in America, but we have come a long way in correcting that problem. Please don’t be one to help perpetuate the “systemic racism” false claims. That only sets us back.
I”m a bit confused about the Bernie bit of your article. I think Bernie is a sincere man, and I’ve seen him in videos when he would visit homes in Michigan about water quality. Why did you pull in his name? Why the interpretations on what his wife did and did not say? I don’t think it is fair that you did that.
What’s incredible about this is that Health Canada has absurdly portrayed lead paint as “an American issue” that we don’t have here. I couldn’t fathom how they could take this stance, but this article made me realize that the lead industries work in portraying this as a “black problem” is the reason why. Health Canada’s view is really “We don’t have the same poor black demographics as the US so logically we do not have a lead paint problem.”
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3222495/
Thank you so much for posting this comment here!
Tamara